
Rajsrinivas
@Rajsrinivas_INR
Passionate about Neurointervention, keen to learn, expand, teach and train. Currently, Sr consultant Neurointerventional Surgery at Paras Health
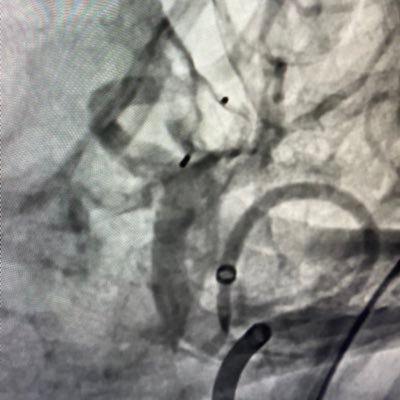
ICAD is always a challenge - Did slow angioplasty over 3 minutes and didn't have the need to drop a stent. Had to retrieve a clot in the inferior division post plasty. Stent in M1 could have posed a problem. Generally gotten away without needing deploy a stent.




Challenging case of aplastic anemia (plt count 6000) not responding to SDAP x 3, plt 23k and acute on chronic subdural. Not a surgical candidate despite gross midline shift. Bilateral MMA embolization with glue/ coil occlusion with resolution of midline shift within six days.


Sharing an interesting case of a giant partly thrombosed cavernous ICA aneurysm with long segment proximal stenosis due to mass effect. We were unable to navigate SOFIA-5F across as it was getting stuck at the level distal end of aneurysm. We used a buddy-wire technique wherein…



Left CCA ostial stenosis 7x39 BMS Over supportive V18 wire Tip: 3mm plasty over 0.014, exchange with V18 0.018 wire for support. Stiff wire allows precise placement of stent



Partially thrombosed giant Cavernous ICA with stenosis and multiple aneurysms. Occluded C/L ICA 6x50 device Technique: Double deployment 1- within SOFIA 2- Unsheath SOFIA @ outer wall and pull back. Easy flush sheath promote fibrin strands on device. Walrus to negate flow…


Dissecting R AICA aneurysm; treated by PAO. Good collateral noted post procedure. Using a reverse (gentle) Headway Duo 1.6 F, Synchro 10, balloon in case needed and floating coils from proximal to dissected segment ensures safety of procedure.


A small lobulated ACOM aneurysm with eccentric orientation posed catheterisation challenges. An oblique-tip microcatheter was used to access the sac without a wire, improving procedural safety.



Welcome to the Hybrid Game-Changer: Start in the angio suite – seal the source with MMA glue embolization Roll into neuro OT – scoop the clot via burr hole or craniotomy All in one anesthesia. All in one go.

FD may not be the solution! Bilobed ruptured PICA; PICA originating from the superior part of the sac, perpendicular curve Microcatheter for the larger sac and regular curve for the smaller sac with Eclipse 2L balloon placed from PICA to VA. With drainage necessary, FD avoided.


Aneurysm vs. Anatomy: A dissecting aneurysm in the right P2 PCA in a child. Challenge was posteromedial choroidal artery was arising from its base. Yet, the sac was occluded safely, and the child walked away without deficits. The secret? A clever vascular balance between the…




A rare case of MCA fenestration in a 4-year-old—confirmed on vessel wall MRI and DSA. Stroke culprit? The fenestration itself. No dissection, no thrombus. Just anatomy playing villain. How often do we miss this in pediatric strokes? pubmed.ncbi.nlm.nih.gov/40134310/ @FishingNeurons

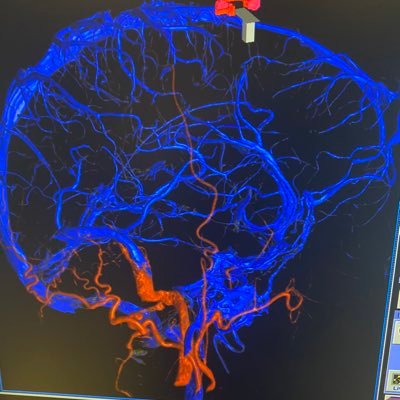
Petrous DAVF with ruptured AICA; Just closing down fistula created natural flow diversion away from AICA aneurysm. This shall promote healing of aneurysm @AshuPJadhav @CanadianNeuroIR @INR_WFITN @INR_WFITN @SVINJournal @slice_inr @CerebrovascLab @UofUNIR @SharathKumarGG7







































































United States Trends
- 1. #BUNCHITA 1,699 posts
- 2. #SmackDown 41.3K posts
- 3. Aaron Gordon 1,578 posts
- 4. Giulia 13.5K posts
- 5. #OPLive 2,174 posts
- 6. Supreme Court 173K posts
- 7. Tulane 3,251 posts
- 8. Caleb Wilson 5,224 posts
- 9. Connor Bedard 1,698 posts
- 10. #BostonBlue 4,155 posts
- 11. #Blackhawks 1,434 posts
- 12. Rockets 19.8K posts
- 13. Northwestern 4,657 posts
- 14. Podz 2,179 posts
- 15. Scott Frost N/A
- 16. Westbrook 4,571 posts
- 17. Lash Legend 5,806 posts
- 18. Chelsea Green 5,844 posts
- 19. Frankenstein 70.3K posts
- 20. Justice Jackson 4,381 posts
Something went wrong.
Something went wrong.